Heart Surgery Risk Estimator
Select options and click Estimate Risk to see results.
Imagine standing in a waiting room, the clock ticking, knowing that the procedure about to happen on your chest or abdomen carries a higher-than-average chance of complications. For most people, "heart surgery" sounds like one thing: bypass grafts or valve replacements. But for surgeons and cardiologists, risk is not a single number. It’s a spectrum. Some operations are routine, with success rates hovering near 98%. Others push the limits of human physiology, where survival depends on millimeters of tissue and minutes of precision.
So, what is the riskiest heart surgery? There isn’t just one answer. The title of "riskiest" usually goes to Redo Heart Surgery, specifically repeat open-heart procedures where scar tissue makes re-entry dangerous, or highly complex repairs like the David Procedure (aortic root replacement with valve preservation) in elderly patients. However, if we look at sheer physiological stress, Heart Transplantation and complex congenital heart defect repairs in adults also top the danger list. The risk depends less on the name of the surgery and more on the patient’s history, age, and how many times their chest has been opened before.
Why Redo Surgery Is Often the Most Dangerous
If you’ve never had heart surgery, your chest cavity is relatively clean. Surgeons can access the heart quickly. But if you’ve had a previous operation-say, a coronary artery bypass graft (CABG) ten years ago-your body has healed over those incisions with dense scar tissue. This tissue sticks to the inside of the breastbone (sternum) and often wraps around major blood vessels, including the aorta and the right ventricle.
When a surgeon needs to open the chest again, they have to cut through this scar tissue. The danger? They might accidentally nick a major vessel. In a first-time surgery, bleeding is manageable. In a redo surgery, it can be catastrophic within seconds. This is why Redo Sternotomy is considered one of the highest-risk maneuvers in cardiothoracic surgery.
- Adhesions: Scar tissue binds organs together, making separation difficult and bloody.
- Vessel Fragility: Previous surgeries can weaken the walls of arteries and veins.
- Time Pressure: Surgeons must work faster to minimize blood loss, which increases the margin for error.
Studies show that mortality rates for redo CABG are significantly higher than for primary CABG. While a first-time bypass might have a mortality rate of 1-2%, a redo procedure can see rates jump to 5-10% or higher, depending on the patient’s overall health. If the patient also needs a new valve replacement during this redo surgery, the complexity-and risk-multiplies.
The David Procedure and Aortic Root Complexity
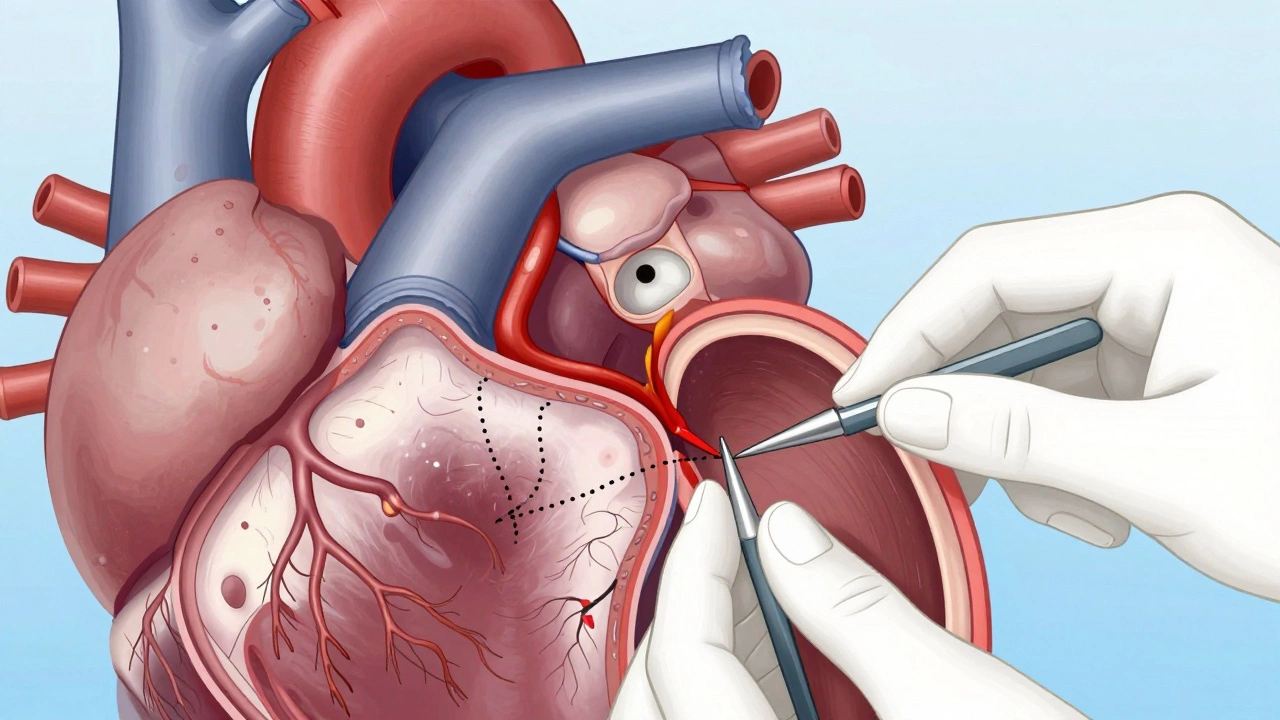
Another contender for the riskiest title is the repair of the aortic root, particularly when preserving the native valve. The aorta is the main highway carrying blood from the heart to the rest of the body. When it dilates (widens) or develops an aneurysm, it threatens to burst.
The David Procedure involves replacing the diseased part of the aorta while keeping the patient’s own aortic valve intact. Unlike simpler replacements where the valve is swapped out entirely, this technique requires intricate sewing inside a beating or stopped heart, under extreme pressure. If the sutures fail, the result is fatal hemorrhage.
This surgery is technically demanding because it combines two high-stakes tasks: vascular reconstruction and valvular repair. It’s often performed on younger patients who want to avoid lifelong blood thinners required by mechanical valves. However, the learning curve for surgeons is steep. In experienced hands, outcomes are excellent. In less experienced centers, the complication rate spikes. For elderly patients with brittle tissues, the risk of tearing the aorta during manipulation is significantly higher.
Heart Transplantation: The Ultimate Physiological Stress
While redo surgery is risky due to anatomy, a Heart Transplant is risky due to systemic failure. By the time a patient qualifies for a transplant, their heart is essentially failing. Their kidneys, liver, and lungs may already be struggling due to poor circulation. Adding the trauma of major surgery to a body that is already on the brink creates a perfect storm.
The surgery itself takes 4-6 hours. During this time, the patient is on a heart-lung machine (cardiopulmonary bypass). Once the new heart is sewn in, it must start beating immediately. Rejection is a constant threat, requiring aggressive immunosuppression that weakens the immune system further. Infections, kidney damage from drugs, and arrhythmias are common post-operative hurdles.
| Surgery Type | Average Mortality Rate (30-day) | Primary Risk Factor | Recovery Time |
|---|---|---|---|
| Primary CABG | 1-2% | Bleeding, infection | 4-6 weeks |
| Redo CABG | 5-10%+ | Scar tissue adhesion, vessel injury | 6-8 weeks |
| Aortic Valve Replacement | 1-3% | Stroke, bleeding | 3-4 weeks |
| Heart Transplant | 5-10% | Organ rejection, multi-organ failure | 3-6 months |
| Complex Congenital Repair | Varies widely (5-20%) | Anatomical complexity, cyanosis | Variable |
Emergency vs. Elective: Timing Changes Everything
A critical factor in determining risk is whether the surgery is planned (elective) or emergency. An elective aortic aneurysm repair has a low risk because the patient is stable, optimized, and prepared. An emergency repair of a ruptured aortic dissection has a mortality rate that can exceed 50%, even with the best surgical team.
In emergency settings, there is no time for pre-habilitation. Patients often arrive in shock, with low blood pressure and organ damage. The surgeon must operate blindly in some cases, dealing with active bleeding and clotting issues. This context turns even routine-looking procedures into life-or-death battles.
Patient-Specific Risks: The STS Score
Surgeons don’t guess risk; they calculate it. The Society of Thoracic Surgeons (STS) National Database uses a risk calculator that inputs dozens of variables: age, weight, kidney function, lung capacity, diabetes status, and prior strokes. A 50-year-old smoker with diabetes facing a redo surgery will have a much higher calculated risk than a 70-year-old non-smoker with good kidney function facing a first-time valve replacement.
This personalized approach means that "the riskiest surgery" is subjective. For a frail 85-year-old, even a simple catheter-based valve replacement (TAVR) carries significant risk. For a healthy 40-year-old, a complex congenital repair might be manageable. Understanding your personal STS score helps set realistic expectations.
How to Mitigate Surgical Risks
Knowing the risks doesn’t mean you should avoid necessary surgery. It means you should prepare aggressively. Here’s how patients can lower their odds of complications:
- Pre-habilitation: Start physical therapy and nutritional support before surgery. Stronger muscles and better protein levels help recovery.
- Smoking Cessation: Quit smoking at least four weeks before surgery. Nicotine constricts blood vessels and impairs healing.
- Diabetes Control: Keep blood sugar levels tight. High glucose increases infection risk dramatically.
- Choose High-Volume Centers: Data consistently shows that hospitals performing more heart surgeries have lower mortality rates. Experience matters.
- Ask About Minimally Invasive Options: For some conditions, smaller incisions reduce trauma and speed up recovery, though not all cases qualify.
Conclusion: Risk Is Manageable, Not Inevitable
The riskiest heart surgeries are those that combine anatomical complexity with patient fragility. Redo surgeries, complex aortic repairs, and transplants sit at the top of the danger list. However, modern medicine has turned many once-fatal procedures into survivable events. By understanding the specific risks associated with your condition and choosing an experienced care team, you can navigate these challenges with confidence.
Is redo heart surgery always more dangerous than the first?
Yes, generally. The presence of scar tissue (adhesions) makes re-entering the chest cavity hazardous. There is a higher risk of injuring major blood vessels or the heart itself during the initial opening of the sternum. Mortality rates are typically 2-3 times higher than primary surgeries.
What is the safest type of heart surgery?
Minimally invasive procedures like TAVR (Transcatheter Aortic Valve Replacement) or PCI (Percutaneous Coronary Intervention/stents) carry the lowest immediate surgical risks because they do not require opening the chest. However, long-term durability varies compared to open surgery.
How does age affect heart surgery risk?
Age is a significant factor. Older patients often have weaker bones, poorer lung function, and more comorbidities like kidney disease. However, biological age matters more than chronological age. A fit 80-year-old may have lower risk than a frail 60-year-old.
Can I reduce my risk before surgery?
Absolutely. Pre-habilitation programs that include exercise, nutrition optimization, smoking cessation, and managing chronic conditions like diabetes can significantly improve surgical outcomes and reduce complication rates.
What is the STS score?
The STS (Society of Thoracic Surgeons) score is a validated risk calculator used by cardiologists and surgeons to predict the likelihood of death or major complications after heart surgery. It considers factors like age, kidney function, ejection fraction, and prior surgeries.